Hair Transplant for Scar Tissue Coverage: The Vascular Biology Decision Framework
Scar tissue is not a monolith. It represents a spectrum of biological environments, each demanding a distinct surgical strategy and a nuanced understanding of vascular biology. For men seeking to address visible scarring from prior hair transplants, accidents, burns, or surgical procedures, the path forward requires more than hope; it requires a clinical framework grounded in science.
The demand for scar revision procedures continues to accelerate. According to the 2025 ISHRS Practice Census, repair procedures rose from 5.4% of all hair transplants in 2021 to 6.9% in 2024. Perhaps more concerning, black-market repair cases nearly doubled during the same period, reaching 10% of all repair cases. These statistics reveal a growing population of men who require specialized intervention from clinicians equipped to handle high-complexity cases.
This article provides a structured, scar-type classification system paired with the vascular biology that governs graft survival. It also examines the regenerative science that is redefining what hair transplantation into scars actually accomplishes. A landmark 2023 study from Imperial College London, published in npj Regenerative Medicine, demonstrated that transplanted follicles do not merely camouflage scar tissue; they actively remodel it. This is not a general overview. It is a clinical decision framework for men who demand precision.
Why Hair Does Not Naturally Regrow in Scar Tissue
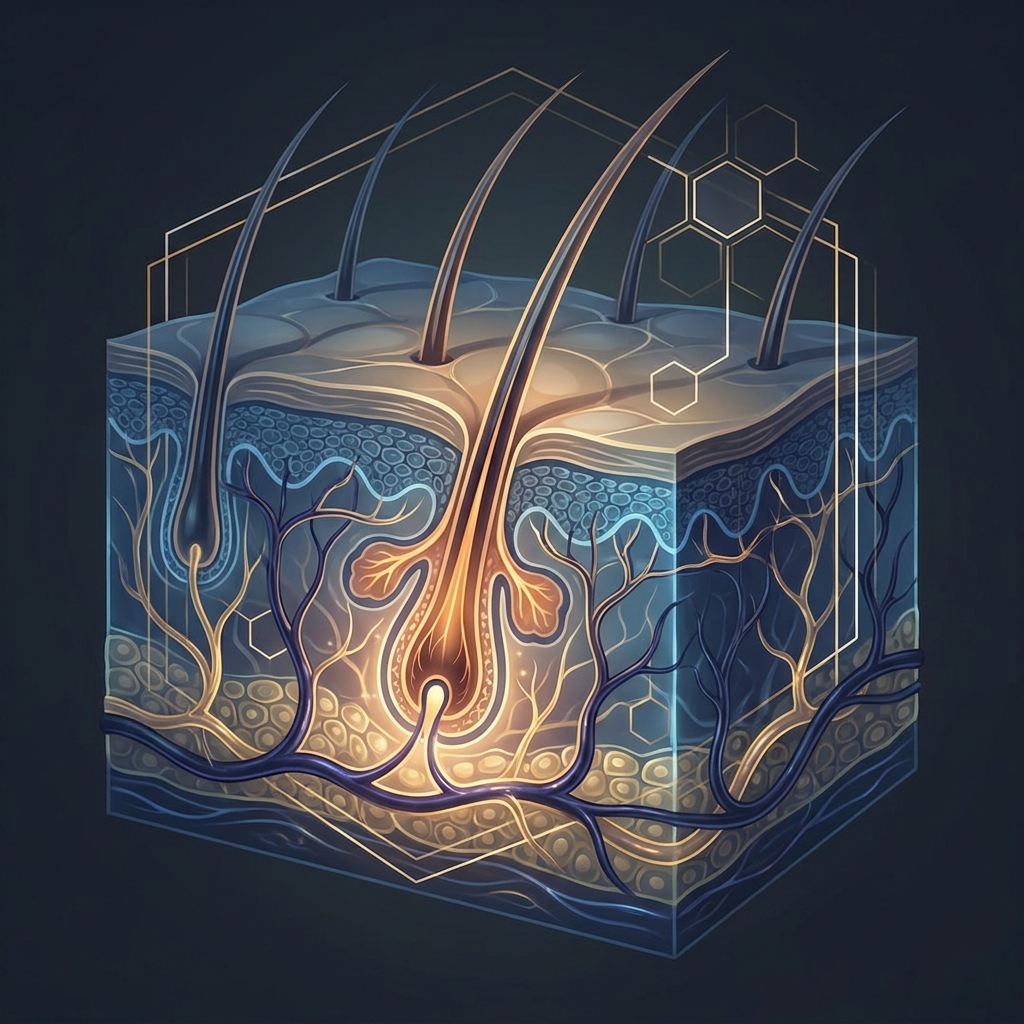
Understanding why hair fails to regenerate in scarred areas is the foundation of any successful treatment strategy. When skin sustains significant injury, the body’s healing response prioritizes closure over restoration. Scar formation destroys original hair follicles and replaces them with dense fibrous collagen, eliminating the structural architecture required for follicular regeneration.
The vascular deficit presents the primary biological challenge. Scar tissue contains significantly fewer capillaries than healthy skin, creating oxygen and nutrient delivery limitations that directly impact graft survival rates. Without adequate blood supply, transplanted follicles cannot establish the connections necessary for sustained growth.
Beyond vascularity, fibrotic collagen cross-linking alters the dermal microenvironment. This disruption interferes with the signaling pathways that sustain the anagen (growth) phase of transplanted follicles. The depth of the scar presents additional complexity: atrophic scars may be too shallow to accommodate the full follicular unit, while hypertrophic scars and keloids present the opposite problem, where implanted follicles may not reach subcutaneous blood supply.
These biological constraints are not insurmountable. They are, however, the prerequisite for selecting the correct technique, density, and pre-conditioning protocol for each scar type.
The Regenerative Science Reframing: Follicles as Active Tissue Remodelers
A paradigm shift occurred in 2023 when researchers at Imperial College London published findings that transformed clinical understanding of scar-coverage transplants. The study, led by Plotczyk et al. and published in npj Regenerative Medicine, demonstrated that transplanted anagen hair follicles actively remodel fibrotic scar tissue.
The findings were significant. Transplanted follicles increased blood vessel density within the scar, reduced pro-fibrotic cytokines including TGFβ1, IL-13, and IL-6, increased epidermal thickness, and enhanced dermal cell density in mature human scar tissue. In essence, hair transplantation into scars functions as a regenerative intervention rather than mere cosmetic camouflage.
The clinical implication is profound. This regenerative remodeling creates a positive feedback loop: as the scar tissue improves following the initial transplant, subsequent graft sessions benefit from a progressively healthier recipient environment. This science forms the foundation of the multi-session, multi-modal approach that defines contemporary scar revision at practices like Hair Doctor NYC.
The Scar-Type Classification System: Five Categories, Five Biological Profiles
Treating scar tissue as a single obstacle leads to suboptimal outcomes. A structured classification system allows surgeons to match biological challenges with precise surgical strategies. Five distinct categories emerge, each with unique vascular, structural, and collagen profiles.
Category 1: FUT Linear Strip Scars
The FUT linear strip scar presents as a single band of fibrotic tissue in the occipital donor zone, typically 1 to 3 mm wide. Capillary density reduction along the scar margin is moderate but consistent. The linear scar creates a predictable dense collagen band where grafts placed too close together compete for limited blood supply.
The recommended strategy involves low-density grafting under 20 grafts per square centimeter using FUE. Mixing scalp hair grafts with the scar’s surrounding native hair achieves seamless blending. The scar’s flat, horizontal orientation requires customized graft angulation to match the natural growth direction of surrounding occipital hair. Surgeons typically begin conservatively and assess survival at 8 to 12 months before adding density in subsequent sessions.
Category 2: FUE Dot Scars (Clustered Micro-Punch Scars)
Multiple small circular scars distributed across the donor zone characterize this category. Each represents a previous FUE extraction site. Individually small, these scars become collectively significant when over-harvested.
Over-harvested donor zones present both individual dot scars and a globally depleted donor supply, limiting available grafts for repair. Individual dot scars can be addressed with single-graft FUE placement. Over-harvested zones may require body hair transplantation using beard, chest, or back hair as supplemental donor sources. Beard hair provides thicker-caliber coverage and high graft survival rates, making it particularly effective for scalp scar coverage when scalp donor supply is exhausted. For patients facing this challenge, understanding options for a hair transplant for thin donor area is an important part of surgical planning.
The 2025 ISHRS Practice Census data showing black-market repair cases at 10% of all repair cases in 2024 reflects the prevalence of severe FUE over-harvesting requiring advanced techniques like body hair transplantation.
Category 3: Burn Scars
Burn scars represent the most vascularly compromised scar type. Extensive fibrosis, severely reduced capillary density, and often irregular surface topography complicate graft placement depth. Without vascular enhancement, graft survival rates are substantially lower than in other scar categories.
The evidence for pre-conditioning is compelling. Research by Ağaoğlu et al. (2021) demonstrated up to 85 to 90 percent graft survival in burn scars pre-treated with fractional CO₂ laser and nanofat injections. Fractional CO₂ laser creates micro-channels that stimulate neovascularization. Nanofat injections deliver adipose-derived stem cells and growth factors that remodel the fibrotic matrix before grafts are placed. Men dealing with this specific challenge can learn more about hair transplant for burn scar scalp coverage as a dedicated treatment pathway.
Burn scar cases typically require the most sessions and the longest inter-session intervals to allow progressive tissue improvement before adding graft density.
Category 4: Trauma and Surgical Scars
Trauma and surgical scars vary considerably depending on mechanism of injury. Accident scars, forehead reduction scars, scalp reduction scars, and post-neurosurgical scars each present different depths, widths, and vascular profiles.
Pre-operative vascular mapping using dermoscopy and Doppler assessment is essential to identify areas of adequate blood supply within irregular trauma scars before planning graft placement. FUE is preferred for its precision and ability to place individual grafts at customized angles and depths.
Trauma scars must be fully mature, typically 9 to 12 months old and ideally 1 to 2 years, before transplantation. Premature intervention into immature scar tissue significantly worsens outcomes. A 2024 randomized controlled trial by Xue et al. demonstrated 82% graft survival in laser-pretreated eyebrow scars versus 74% in untreated scars, validating laser pre-conditioning for non-scalp scar sites.
Category 5: Legacy Cobblestone Plug Scars
The result of outdated large-punch hair plug procedures from the 1970s through 1990s, cobblestone scars present irregular, raised, or depressed scar clusters with unpredictable vascular architecture between plug sites.
Surgeons must simultaneously camouflage the unnatural plug appearance and address the fibrotic tissue between plugs. The surgical strategy involves FUE placement between existing plugs at low density, combined with scalp micropigmentation to blend color and reduce the visual contrast of the cobblestone texture.
Cobblestone plug patients often carry decades of self-consciousness about their appearance. Setting realistic expectations about the multi-session nature of revision is essential to patient satisfaction.
Graft Survival Rates in Scar Tissue: What the Data Actually Shows
Graft survival in healthy scalp reaches 90% or higher with a skilled surgeon. In scar tissue, survival rates typically range from 66 to 81 percent depending on scar type, pre-treatment, and surgeon expertise.
The survival rate spectrum by scar type reveals important patterns: burn scars with pre-conditioning achieve 85 to 90 percent (Ağaoğlu 2021), laser-pretreated scars reach 82 percent (Xue 2024 RCT), FUE-treated scar tissue generally achieves approximately 81 percent, and untreated scars fall to 74 percent or lower.
Three primary variables determine survival: capillary density at the recipient site, the pre-conditioning protocol employed, and the surgeon’s graft density discipline. Surgeons must space grafts further apart in scar tissue than in healthy scalp to ensure adequate blood flow to each follicle. Over-packing grafts into compromised tissue directly reduces survival rates.
Lower initial survival rates are not a failure. They represent the biological reality of the first session. Subsequent sessions in progressively remodeled tissue typically achieve higher survival rates.
Pre-Operative Optimization: Preparing Scar Tissue for Transplantation
Pre-conditioning represents the difference between adequate and excellent outcomes. The biological environment at the time of transplantation is as important as surgical technique.
Fractional CO₂ laser pre-conditioning creates controlled micro-injury that stimulates neovascularization and collagen remodeling, improving capillary density before grafts are placed. The Xue 2024 RCT demonstrated 82% versus 74% survival with this approach.
PRP (Platelet-Rich Plasma) serves as a powerful adjuvant. A 2025 PRISMA-compliant systematic review confirms PRP promotes neovascularization, enhances graft survival, and improves the microenvironment of transplanted areas. Johns Hopkins Medicine confirms PRP stimulates hair growth after transplants. Patients interested in this adjuvant therapy can explore how platelet-rich plasma can change your hair as part of a comprehensive scar revision protocol.
Topical minoxidil application at 2 to 5 percent concentration for one week before and five weeks after surgery has been suggested to improve blood supply and graft survival in scar tissue. Combined PRP plus microneedling has proven safe and effective, with a 2025 peer-reviewed study of 107 scar patients finding the most frequent outcome to be softer, more flexible scar tissue.
The scar maturity requirement remains non-negotiable. Scars must be 9 to 12 months old at minimum, ideally 1 to 2 years, before transplantation.
Contraindications: When Scar Tissue Transplantation Is Not Appropriate
Keloid-prone patients present the highest surgical risk. Implanted follicles may not reach adequate depth to access subcutaneous blood supply, and surgical trauma can reactivate dormant keloid formation.
Patients with active inflammatory scarring diseases, including lichen planopilaris and discoid lupus erythematosus, are poor candidates. The disease must be quiescent for at least 1 to 2 years before surgery is considered. Operating on scars less than 9 to 12 months old introduces grafts into an unstable inflammatory environment where ongoing remodeling actively impairs graft survival.
These contraindications are not always apparent to patients or general practitioners. Understanding hair transplant candidacy criteria is essential, and a surgeon with specific scar revision expertise is required to accurately assess candidacy.
The Multi-Modal Gold Standard: Combining FUE, SMP, and Regenerative Adjuvants
The combination protocol representing the current clinical standard of care for scar revision integrates FUE transplantation into the scar with scalp micropigmentation for color blending and PRP/microneedling for tissue quality optimization.
SMP creates the appearance of hair follicles between transplanted grafts, reducing the visual contrast of the scar during the growth phase and providing a permanent complementary solution for areas where graft density is limited by vascular constraints. Pigment spreading and fading are less predictable on scar tissue than on healthy skin, requiring physician supervision and specialized technique.
PRP and microneedling bridge sessions, continuing the tissue remodeling process initiated by the transplanted follicles. Most scar coverage cases require multiple sessions with 8 to 12 months between each. This is not a limitation but a biological necessity that allows progressive tissue improvement and accurate survival assessment before adding density. Thoughtful hair transplant multi-procedure planning is therefore central to achieving optimal long-term results.
Why Specialist Selection Is the Most Important Variable
The surgeon selection decision represents the single highest-impact variable in scar tissue transplant outcomes. The near-doubling of black-market repair cases from 6% to 10% of all repair cases between 2021 and 2024 demonstrates the real-world consequences of inadequate specialist selection.
Scar-specific expertise requires experience with vascular assessment of recipient sites, proficiency in low-density graft placement discipline, familiarity with pre-conditioning protocols, and the judgment to stage procedures appropriately.
The value of a multi-modal team cannot be overstated. The combination of FUE surgical expertise, SMP specialization, and regenerative adjuvant capability under one clinical roof eliminates the coordination failures that occur when patients seek these services from separate providers.
Hair Doctor NYC’s team credentials reflect this precise combination of expertise. Dr. Roy B. Stoller’s 6,000-plus procedures and 25-plus years of experience in facial plastic surgery and hair restoration, Dr. Christopher Pawlinga’s 18 years of exclusive hair transplant focus, and Michael Ferranti’s 25-plus years in aesthetic dermatology with licensed SMP specialization represent the multi-disciplinary approach scar revision cases demand.
Conclusion: Scar Tissue Is a Biological Challenge, Not a Barrier
Scar tissue presents a spectrum of vascular and structural challenges. With the correct classification, pre-conditioning, surgical technique, and multi-modal protocol, hair transplantation into scars is not only possible but regeneratively transformative.
The Imperial College London finding remains the defining scientific insight: transplanted follicles actively remodel fibrotic tissue, meaning each session improves the biological environment for the next. Scar revision is a progressive regenerative process, not a single cosmetic intervention.
Graft survival rates in scar tissue range from 66 to 90 percent depending on type and pre-conditioning, which is lower than in healthy scalp. Multiple sessions are the norm, and outcomes depend heavily on surgeon expertise and patient candidacy. As ISHRS 2025 data confirms, repair procedures are the fastest-growing segment of hair restoration. Patients deserve access to clinicians who treat scar revision as the specialized discipline it is.
For men who carry the visible evidence of prior procedures, accidents, or burns, the science of today offers a genuinely regenerative path forward.
Schedule Your Scar Tissue Consultation at Hair Doctor NYC
Men seeking to address visible scarring are invited to schedule a personalized consultation with the Hair Doctor NYC team. A specialist evaluation will determine scar maturity, vascular adequacy, pre-conditioning requirements, and a realistic multi-session roadmap.
Hair Doctor NYC’s team provides the full multi-modal scar revision protocol under one roof on Madison Avenue in Midtown Manhattan. With a track record of 6,000-plus successful procedures and the “Excellence Meets Elegance” standard of care, the practice represents the specialist resource for high-complexity scar revision cases in New York.
Contact Hair Doctor NYC at hairdoctornyc.com to schedule a confidential, personalized scar tissue assessment with the clinical team.