Alopecia Areata Treatment Options Overview: The Severity-Staged Decision Framework
Alopecia areata affects approximately 2% of the global population over a lifetime, yet the decisions surrounding its treatment remain poorly understood by most people living with it. A patient who searches for answers typically encounters a flat list of options: corticosteroids, minoxidil, JAK inhibitors, immunotherapy. What almost no one provides is the more important information: which of those treatments actually applies to a specific presentation, at a specific disease stage, for a specific person.
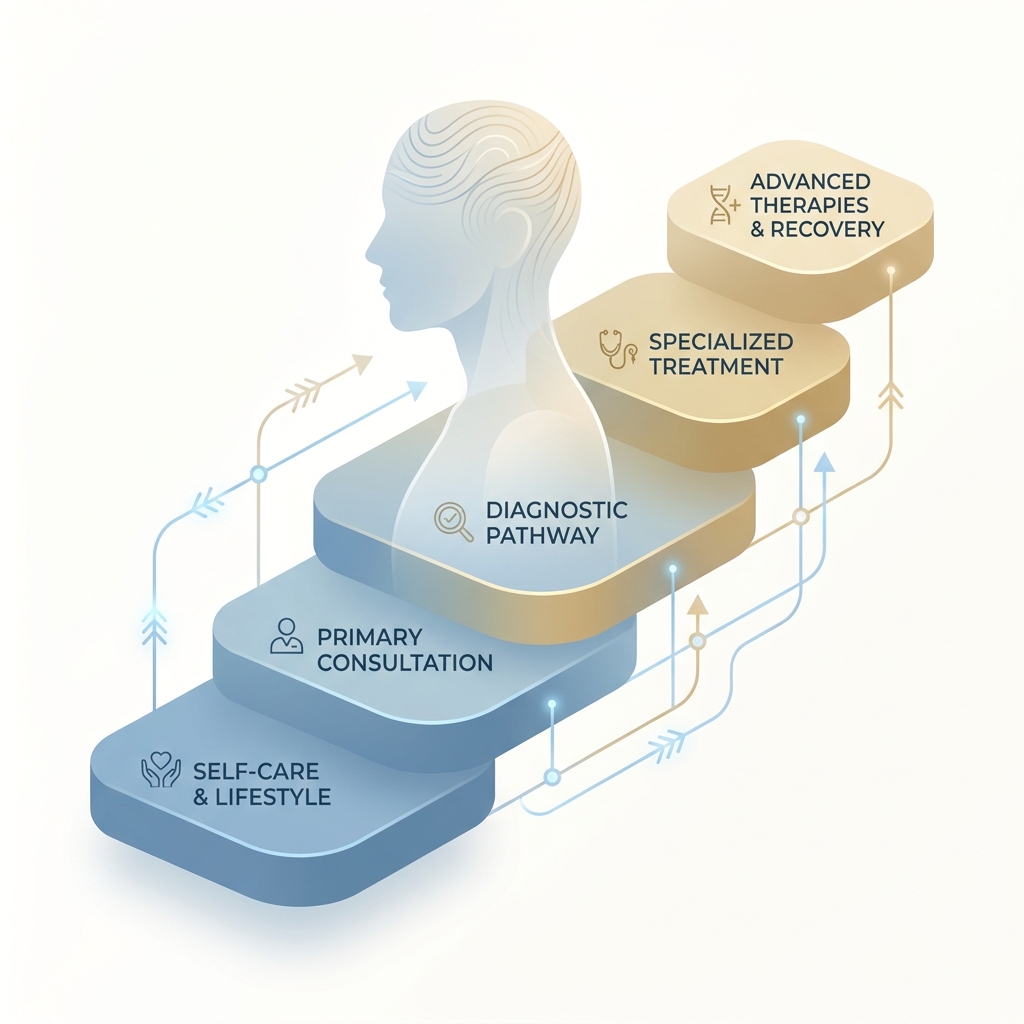
That gap is the problem this article solves. Treatment decisions in alopecia areata are not one-size-fits-all. They map directly to disease presentation, SALT score, duration, rate of progression, and psychosocial impact. Understanding this severity-staged framework transforms a confusing menu into a logical decision pathway.
The timing matters. Until 2022, there were no FDA-approved disease-modifying systemic treatments for this condition. Today there are three. That is one of the most significant shifts in the history of dermatologic care, and it has changed what is possible for patients with severe disease.
What follows is a clinically grounded walk through each treatment tier, from watchful waiting through systemic therapy. It addresses the honest science behind why hair transplant is contraindicated in most cases, and it treats the psychosocial dimension (which affects nearly 60% of patients) as the primary clinical concern it is.
Understanding Alopecia Areata Before Choosing a Treatment
Alopecia areata is a chronic autoimmune condition in which CD8 T-cells attack the hair follicles. The attack is driven by the cytokines interferon-gamma and interleukin-15, which is precisely why inhibition of the JAK-STAT signaling pathway has become the most targeted therapeutic approach available. Blocking that pathway interrupts the signal the immune system uses to sustain its assault on the follicle.
Critically, alopecia areata is a non-scarring form of hair loss. The follicles are damaged but not destroyed. That distinction matters enormously, because it means regrowth is biologically possible in most cases. The follicle is dormant, not dead.
The condition presents in three major clinical forms. Patchy alopecia areata is the most common, producing discrete round or oval bald patches. Alopecia totalis involves complete loss of scalp hair. Alopecia universalis involves total loss of hair across the entire body. Progression to totalis or universalis occurs in up to 10% of all cases, and spontaneous remission in these severe subtypes is uncommon.
Clinicians measure severity using the SALT score, or Severity of Alopecia Tool, which runs from 0 (no hair loss) to 100 (complete scalp hair loss). A SALT score of 50 or greater is generally considered severe disease. Patients should understand this number, because it directly determines treatment eligibility, particularly for systemic therapy.
The spontaneous remission data deserves attention up front. According to a review published in PMC, remission rates run as high as 68% in patients with less than 25% scalp involvement, but drop to only 8% in those with greater than 50% involvement. Within 20 years, essentially all patients experience some disease relapse. This is why remission data drives treatment decisions: mild disease may resolve on its own, while severe disease almost certainly will not.
How Disease Severity Drives Treatment Selection
Treatment in alopecia areata is not chosen arbitrarily. It follows a logical algorithm based on the extent of hair loss as measured by SALT score, the duration of the disease, the rate of progression, the presence or absence of inflammation on biopsy, and the psychosocial burden the patient carries. The framework presented here reflects current international guideline consensus, as summarized in a 2025 comparison of international management guidelines, and the clinical approach used at specialist practices.
Five tiers follow: watchful waiting, topical and intralesional corticosteroids, contact immunotherapy, JAK inhibitor therapy, and scalp micropigmentation. Hair transplant is addressed separately, as a narrow exception rather than a standard tier.
Patient selection is crucial at every level. The best candidates for systemic therapy, for example, typically have 50% or greater scalp hair loss, disease duration under 10 years, and significant psychosocial impact. One truth applies across the entire framework: no treatment currently cures alopecia areata. All therapies manage the condition, and relapse remains a defining feature of the disease.
Tier 1: Watchful Waiting, When Observation Is the Right Clinical Choice
Watchful waiting is a legitimate, evidence-informed clinical decision. It is not inaction, and it is not neglect.
The appropriate candidate has patchy disease involving less than 25% of the scalp, recent onset, no rapid progression, and a high probability of spontaneous remission. Given that up to 68% of patients with limited disease experience spontaneous regrowth, initiating aggressive treatment in this group may expose a patient to side effects without meaningful benefit over the disease’s natural course.
Monitoring during this period is active, not passive. It includes regular clinical assessment, SALT score tracking, dermoscopy to evaluate follicular inflammation, and psychosocial check-ins. Watchful waiting is not indefinite delay. If the disease progresses beyond 25% to 30% scalp involvement, or shows no signs of remission within a defined observation window, escalation is warranted.
The clinical rationale is sound: intervening in disease that would likely resolve on its own can do more harm than good. As Medscape notes in its treatment guidance, treatment of alopecia areata is not mandatory, because the condition is benign, and spontaneous remissions and recurrences are common.
Tier 2: Topical and Intralesional Corticosteroids, First-Line Therapy for Localized Disease
Corticosteroids are the established first-line treatment for mild to moderate, localized alopecia areata, supported by decades of clinical use. As noted in a 2025 JAAD clinical review, topical and intralesional corticosteroids remain first-line for mild or localized disease, though their efficacy can be inconsistent and relapse is common. The mechanism is straightforward: corticosteroids suppress local immune activity around the follicle, reducing the autoimmune attack.
Topical Corticosteroids
High-potency topical steroids, such as clobetasol propionate, are applied directly to affected patches. They are appropriate for superficial, limited patches, for patients who cannot tolerate injections, and as an adjunct alongside other therapies.
The limitations are real. Efficacy is inconsistent, prolonged use carries a risk of skin atrophy, and relapse is common once the patient stops applying the medication. Topical minoxidil is frequently used as an adjunct to enhance follicular response. It is not a standalone treatment for alopecia areata, but it is a useful combination agent.
Intralesional Corticosteroid Injections
Triamcinolone acetonide injected directly into affected scalp patches is the most commonly used and best-studied approach for localized disease. It is appropriate for stable, patchy alopecia areata with defined areas of involvement, generally in patients with SALT scores below 50.
The approach produces regrowth in a meaningful proportion of patients with limited disease, though response varies. It requires repeated office visits, typically every four to six weeks, and it is not practical for extensive or rapidly progressing disease. Intralesional steroids do not modify the underlying autoimmune process, so relapse is common. They are not appropriate for alopecia totalis or universalis, where the treatment burden would be prohibitive and efficacy is poor.
Tier 3: Contact Immunotherapy, An Underutilized Option for Moderate Disease
Contact immunotherapy, using agents such as diphencyprone (DPCP) or squaric acid dibutyl ester (SADBE), is a second-line option for patients who have not responded to corticosteroids or who have more extensive patchy disease.
The mechanism is elegant. A sensitizing agent applied to the scalp provokes a controlled allergic reaction that is thought to redirect the immune attack away from the hair follicles, functioning as an immunological distraction strategy. Response rates in the literature range broadly, with some studies showing regrowth in 40% to 60% of appropriately selected patients. Results are more favorable in patchy disease than in totalis or universalis.
Practical considerations apply. Treatment requires careful dose titration, regular clinic visits, and patient tolerance of a mild inflammatory scalp reaction. It is used off-label, requires specialist administration, and response can take months. Relapse after discontinuation is common.
This tier deserves emphasis because many patients are never offered it. For a patient with moderate disease who wants to exhaust non-systemic options before committing to JAK inhibitor therapy, contact immunotherapy is an important consideration. Patients navigating this decision may also benefit from reviewing a non-surgical hair restoration treatment hierarchy to understand how these options fit within the broader landscape.
Tier 4: JAK Inhibitor Therapy, The Transformational Advance for Severe Alopecia Areata
As HCPLive noted in 2026, the approval of three JAK inhibitors represents a transformational moment in a field that until very recently had no reliable disease-modifying systemic options.
The mechanism is the most targeted approach currently available. JAK inhibitors block the JAK-STAT signaling pathway that interferon-gamma and interleukin-15 use to drive the autoimmune attack on hair follicles. Interrupting that signal allows the follicle to recover.
The Three FDA-Approved JAK Inhibitors: Profiles and Distinctions
According to the National Alopecia Areata Foundation, three JAK inhibitors are now approved:
- Baricitinib (Olumiant): FDA-approved in 2022 for adults 18 and older. Phase 3 trials demonstrated 35% to 40% of patients achieving a SALT score of 20 or less at 36 weeks, per a 2025 narrative review in PMC. It was the first approval and remains the most studied.
- Ritlecitinib (Litfulo): FDA-approved in 2023. It is the only JAK inhibitor approved for adolescents ages 12 and older, which matters for families navigating pediatric disease.
- Deuruxolitinib (Leqselvi): FDA-approved for adults and commercially launched on July 14, 2025. As the newest entrant, it is differentiated by rapid onset and sustained efficacy in 2025 to 2026 clinical reviews, representing the current leading edge of approved therapy.
All three have demonstrated efficacy in Phase 3 trials. The choice between them involves patient-specific factors including age, comorbidities, and response profile, and it is a decision made in consultation with a specialist.
Who Is an Appropriate Candidate for JAK Inhibitor Therapy
Appropriate candidates are adults with severe disease (SALT 50 or greater), alopecia totalis, or alopecia universalis who have failed or are not candidates for first- and second-line therapies. The best-response profile includes disease duration under 10 years, significant psychosocial impact, and no contraindications to systemic immunosuppression.
The pre-treatment workup is standard and thorough: screening for infections including tuberculosis and hepatitis, baseline laboratory tests, and cardiovascular risk assessment. Patients with a history of malignancy, active serious infections, or certain cardiovascular risk factors require careful evaluation before initiation.
The Boxed Warning and Safety Profile: What Patients Must Understand
All three approved JAK inhibitors carry a class-wide boxed warning for serious infections, malignancy, major adverse cardiovascular events, and thrombosis. The critical context is that Phase 3 trials in alopecia areata have not demonstrated unexpected safety signals at the doses used for this condition. The boxed warning is a class label derived largely from higher-dose use in rheumatoid arthritis populations.
That does not mean the risks are absent. It means they must be discussed, monitored for, and weighed against the severity of disease and its impact on quality of life. Regular monitoring through labs and clinical assessment is required throughout treatment. This is not a set-and-forget therapy; it is an ongoing clinical relationship.
The Relapse Reality: What Happens When JAK Inhibitors Are Discontinued
This is the most important fact many patients never receive before starting treatment: discontinuation is associated with relapse. Hair loss recurs in the majority of patients who stop the medication. Long-term, likely indefinite treatment is often necessary to maintain regrowth, because JAK inhibitors suppress the autoimmune process but do not cure it.
Patients must understand this before committing. JAK inhibitor therapy is a long-term management strategy, not a finite course. That reality carries practical implications for health management, monitoring schedules, and sustained commitment. For patients with severe disease whose quality of life is significantly affected, the benefit-to-burden ratio often strongly favors treatment. Informed consent, however, requires full transparency about the long-term nature of the commitment.
Tier 5: Scalp Micropigmentation, A Non-Surgical Solution for Appearance and Confidence
Scalp micropigmentation (SMP) occupies a distinct tier. It is not a medical treatment for the autoimmune process. It is a highly effective non-surgical cosmetic solution that addresses the visible and psychosocial impact of the condition.
The procedure applies medical-grade pigments to the scalp to replicate the appearance of hair follicles, creating the visual effect of a closely cropped or shaved head. In the context of alopecia areata, appropriate candidates include patients with extensive or total hair loss who are not candidates for (or not interested in) systemic therapy, patients awaiting response to medical treatment, and those who want to address their appearance while managing the underlying condition medically.
The key advantage over hair transplant is significant. SMP does not involve any manipulation of the follicle, carries no risk of triggering disease flares, and is not contraindicated by active disease. For a patient experiencing the identity and confidence impact of significant hair loss, scalp micropigmentation for alopecia areata can deliver an immediate, meaningful improvement in appearance and self-perception while medical management continues.
At Hair Doctor NYC, scalp micropigmentation is performed by Michael Ferranti, P.A., a licensed SMP specialist with more than 25 years of experience in aesthetic dermatology and plastic surgery, ensuring clinical-grade precision and natural results.
Hair Transplant and Alopecia Areata: The Honest Science
Hair transplant is generally contraindicated in active alopecia areata. That is the clinical consensus, and patients deserve to understand exactly why.
Why Hair Transplant Fails in Active Alopecia Areata: The Mechanism
There are three core reasons.
The autoimmune attack continues after transplant. Moving follicles into an affected scalp does nothing to change the underlying immune environment. The same CD8 T-cell attack that caused the original hair loss will target the transplanted grafts.
There is no safe donor zone. In androgenetic alopecia, donor follicles from the occipital scalp are genetically resistant to DHT and reliably survive transplantation. In alopecia areata, all follicles (including those at the donor site) are susceptible to the autoimmune attack. There is no reliably safe source of grafts.
Disease reactivation is a documented risk. The trauma of follicular extraction and implantation can trigger disease flares, accelerating hair loss in both the recipient and donor areas.
Transplanting into an active autoimmune environment risks graft failure, donor site damage, and disease exacerbation. It is not a viable strategy.
The Narrow Exception: When Transplant May Be Reconsidered
In very rare, highly selected cases, transplant may be considered, but the bar is high. The stability criteria that must be met include: disease that has been clinically stable for a minimum of two to three years with no new patches or progression; a scalp biopsy showing no active perifollicular inflammation; small and defined, unchanged patches rather than diffuse loss; and high-quality donor follicles with no clinical evidence of disease involvement.
Even when all criteria are met, outcomes remain unpredictable. The autoimmune process can reactivate at any time, including after transplant. This is not a decision made lightly or quickly. It requires thorough specialist evaluation and realistic expectation-setting. Patients considering this path should review the detailed alopecia areata hair transplant candidacy criteria before proceeding.
The team at Hair Doctor NYC is uniquely qualified to make this nuanced assessment. With over 6,000 procedures performed by Dr. Roy B. Stoller and decades of specialized experience across the practice, the clinical depth exists to evaluate whether a patient truly meets the narrow exception criteria for transplant consideration, along with the integrity to advise against transplant when they do not.
The Psychosocial Dimension: Treating the Whole Patient
Psychological distress affects nearly 60% of patients with alopecia areata. This is not a secondary concern; it is a primary clinical finding that must be addressed alongside physical treatment.
Research published in the British Journal of Dermatology in 2025 found that the psychosocial burden is more strongly linked to illness perceptions and stigma than to objective disease severity. In practical terms, a patient with limited patchy disease may experience greater distress than one with more extensive loss, depending entirely on how the condition is perceived and internalized.
Anxiety-related disorders are more prevalent among patients than in the general population, and depression, social withdrawal, and occupational impact are documented consequences. Hair loss can intersect with identity, professional confidence, and social presence in ways that are not always easy to articulate. A specialist practice should create space for these conversations without minimizing them.
Psychosocial assessment therefore belongs in every evaluation, not as an afterthought. Treatment decisions should account for quality-of-life impact, not just the SALT score. Patients experiencing significant distress should consider working with a mental health professional alongside their dermatologic or hair restoration specialist; these are complementary interventions, not competing ones. SMP, medical therapies, and specialist consultation all contribute to psychosocial recovery by restoring a sense of agency and control over one’s appearance.
Emerging Treatments: What Is on the Horizon for Alopecia Areata
The pipeline is genuinely active for patients who want to understand where the field is heading.
Rezpegaldesleukin is a Treg-mechanism biologic that completed its Phase 2b REZOLVE-AA trial with proof-of-concept established and is advancing into Phase 3 as a potential first-line treatment for severe-to-very-severe disease. It is notable because it works through a fundamentally different mechanism than JAK inhibitors, expanding regulatory T-cells rather than inhibiting the JAK-STAT pathway.
Upadacitinib, a JAK inhibitor currently in Phase 3 trials, may offer an additional approved option with a distinct selectivity profile.
Dupilumab has shown 48% to 97% improvement in patients with comorbid atopic dermatitis, making it a logical choice for the subset of patients who also have eczema or other atopic conditions where the inflammatory overlap is relevant.
Topical JAK inhibitors are in investigational development, aiming to deliver JAK inhibition locally without systemic exposure, which could matter significantly for patients who are not candidates for oral therapy.
The landscape is evolving rapidly. Patients who are not responding to current options, or who are not yet candidates for approved therapies, may have meaningful new options within the next two to four years. Staying engaged with a specialist practice ensures access to those options as they become available.
Navigating Insurance and Access to JAK Inhibitor Therapy
Access to JAK inhibitor therapy remains a significant real-world barrier for many patients, with access surveys documenting disparities in timely care. Prior authorization requirements, step therapy protocols, and formulary restrictions can delay access to approved therapies, and patients should be prepared for that process.
A specialist practice provides real leverage here. The clinical documentation, SALT score assessments, and prior treatment history needed to support insurance authorization are precisely what a specialist’s office produces. Patient assistance programs also exist through the manufacturers of all three approved JAK inhibitors, and a specialist’s office can help navigate them. The National Alopecia Areata Foundation maintains credible resources to help patients understand their options and navigate these challenges.
The Severity-Staged Framework at a Glance
The full decision framework, in scannable form:
- Mild / Limited Patchy AA (SALT under 25%): Watchful waiting with monitoring; topical or intralesional corticosteroids as first-line intervention; topical minoxidil as adjunct.
- Moderate Patchy AA (SALT 25% to 49%, corticosteroid non-response): Contact immunotherapy (DPCP or SADBE); continued intralesional corticosteroids; psychosocial assessment and support.
- Severe AA / Alopecia Totalis / Alopecia Universalis (SALT 50% or greater): JAK inhibitor therapy (baricitinib, ritlecitinib for ages 12 and up, or deuruxolitinib for adults) following appropriate screening; SMP as a complementary non-surgical option for appearance management.
- Hair Transplant: Not indicated in active disease; narrow exception criteria apply only after two to three or more years of documented stability, negative biopsy for inflammation, and specialist evaluation.
- Psychosocial Support: Integrated at every tier, not reserved for severe disease.
This framework is a clinical guide, not a self-diagnosis tool. Individual patient factors, comorbidities, and disease trajectory require specialist evaluation to apply correctly.
Conclusion: Alopecia Areata Is Manageable With the Right Framework and the Right Specialist
Alopecia areata is a complex, chronic autoimmune condition. It is not, however, untreatable. The landscape has changed dramatically with the approval of three JAK inhibitors since 2022, giving patients with severe disease real, evidence-based options where none existed before.
The honest complexity remains. No treatment cures the condition, relapse is a defining feature, and effective treatment requires careful matching of therapy to disease presentation. Patients who understand their disease stage, their SALT score, and their options are far better equipped to have productive conversations with their specialist and make informed decisions.
The physical and psychological dimensions of this condition are inseparable, and a practice that addresses both is better positioned to deliver meaningful outcomes. The pipeline is active, the science is advancing, and patients who stay engaged with a specialist will have access to emerging options as they arrive.
Schedule a Consultation at Hair Doctor NYC
The logical next step is a consultation with the specialist team at Hair Doctor NYC on Madison Avenue in Midtown Manhattan. This is a clinical evaluation, not a sales conversation. The goal is an accurate assessment of disease stage, treatment history, and appropriate next steps.
The team’s qualifications map directly to the demands of this condition. Dr. Roy B. Stoller brings more than 25 years of experience and over 6,000 procedures performed. The practice offers a comprehensive approach spanning medical evaluation, scalp micropigmentation, and surgical options, along with the clinical depth to make the nuanced determination of whether a patient meets the narrow exception criteria for transplant consideration.
That whole-patient philosophy, combining clinical expertise with a genuine understanding of the psychosocial impact of hair loss, reflects the Excellence Meets Elegance standard that defines the practice. Every evaluation is handled with the discretion and personalization that discerning patients expect.
Contact Hair Doctor NYC to schedule a comprehensive alopecia areata evaluation and begin building a treatment plan tailored to a specific disease presentation.